Music can have a tremendous impact on healthy aging – most critically, a person’s cognitive health. It can be the best medicine, and unlike nearly any other medication, it has no bad side effects.

More and more physicians are signing employment contracts as opposed to opening up a practice. If you see any of these 8 concerning contract items when reviewing your contract, it is probably time to negotiate.

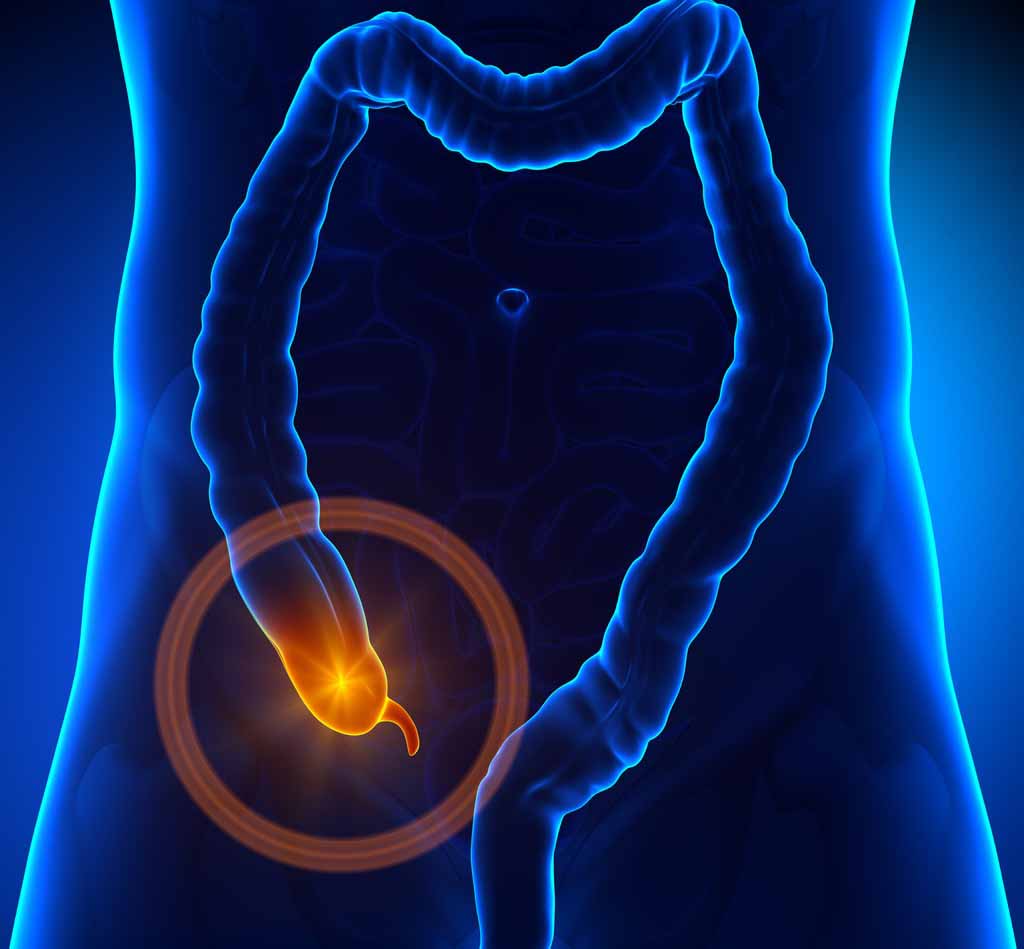
A Physician faces his own diagnostic failure when it counts the most. A minor surgery is always something that happens to someone else.
Founded in 2005, The Doctor Weighs In has grown into a multimedia company with millions of readers around the world.
 Trusted content written and reviewed by doctors and other experts
Source for reliable information about emerging health and wellness technologies
Trusted content written and reviewed by doctors and other experts
Source for reliable information about emerging health and wellness technologies 





Is a physician executive and health journalist who founded and serves as the CEO and Editor-in-Chief of The Doctor Weighs In. She was a double-boarded emergency physician at Kaiser Permanente until transitioning into a national executive position as the organization’s first Director of National Accounts. Over the course of her career, she has worked in leadership roles in almost every aspect of healthcare. She has also been a Top Voice in Healthcare on LinkedIn for 2017 and 2018. Learn more here.